Skip to main content
Hit enter to search or ESC to close
New Clients
Practice Policies
Take A Tour
Pet Insurance
About Us
Career Opportunities
Services
Surgical Services
Medical Services
Anesthesia and Patient Monitoring
Preventive Services
Wellness and Vaccination Programs
Additional Services
Wellness Plans
Canine Plans
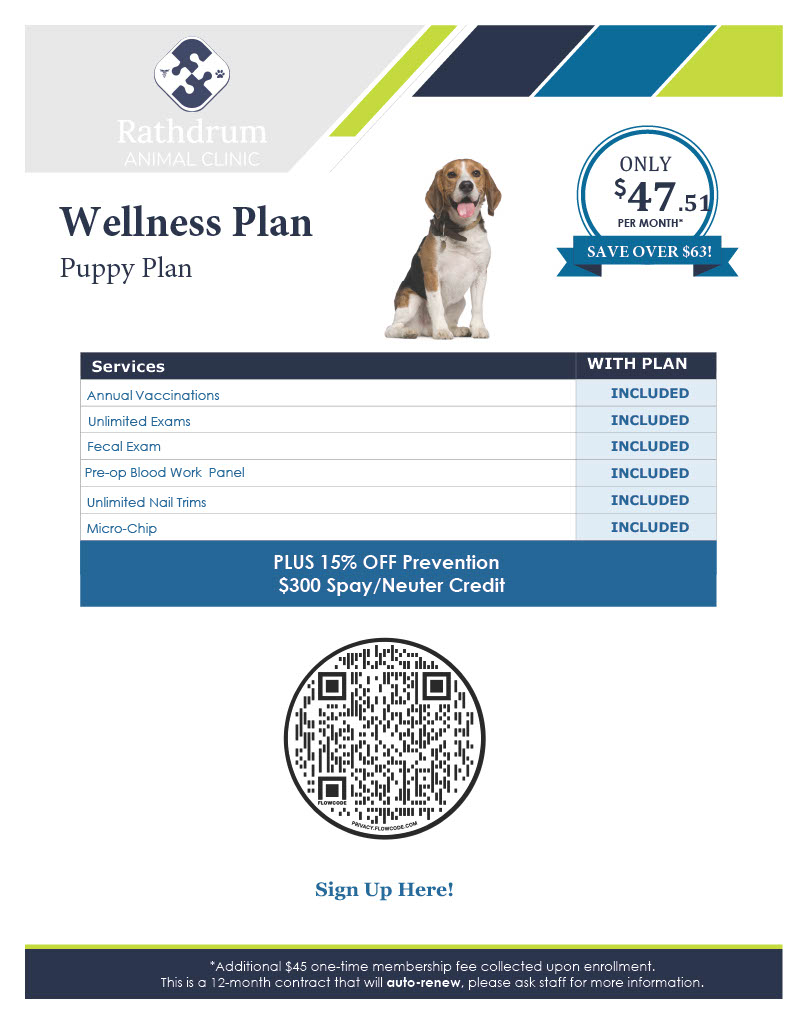
Puppy Plan
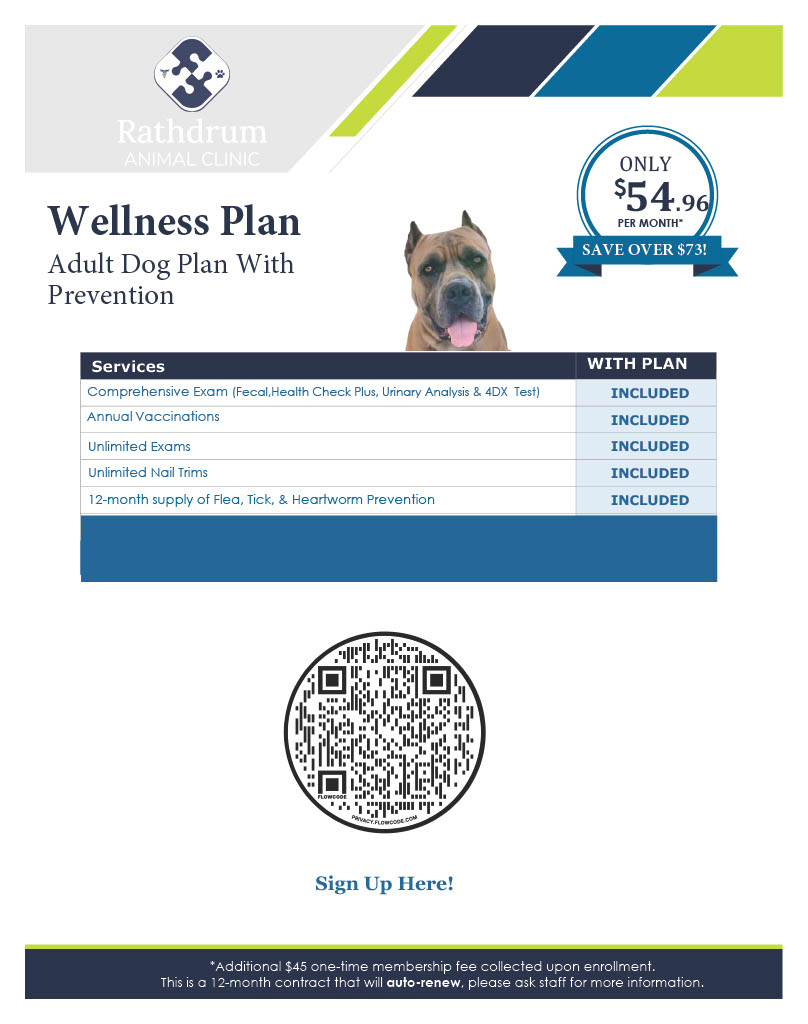
Adult Plan w/ Prevention
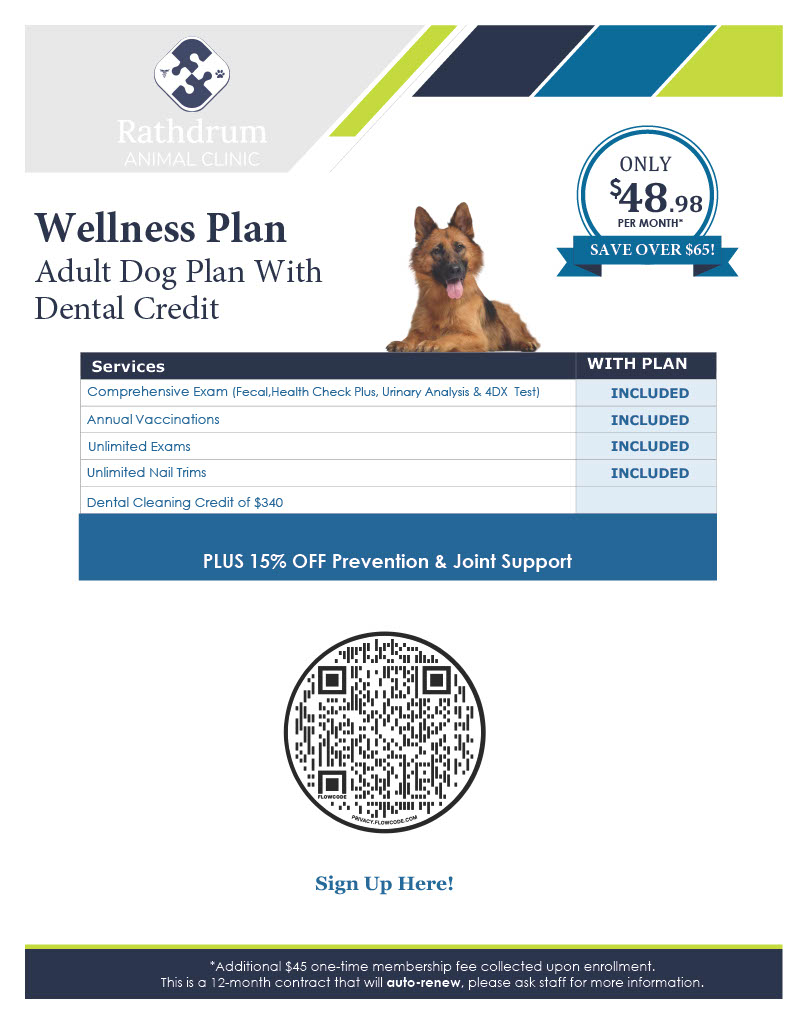
Adult Plan w/ Dental Credit
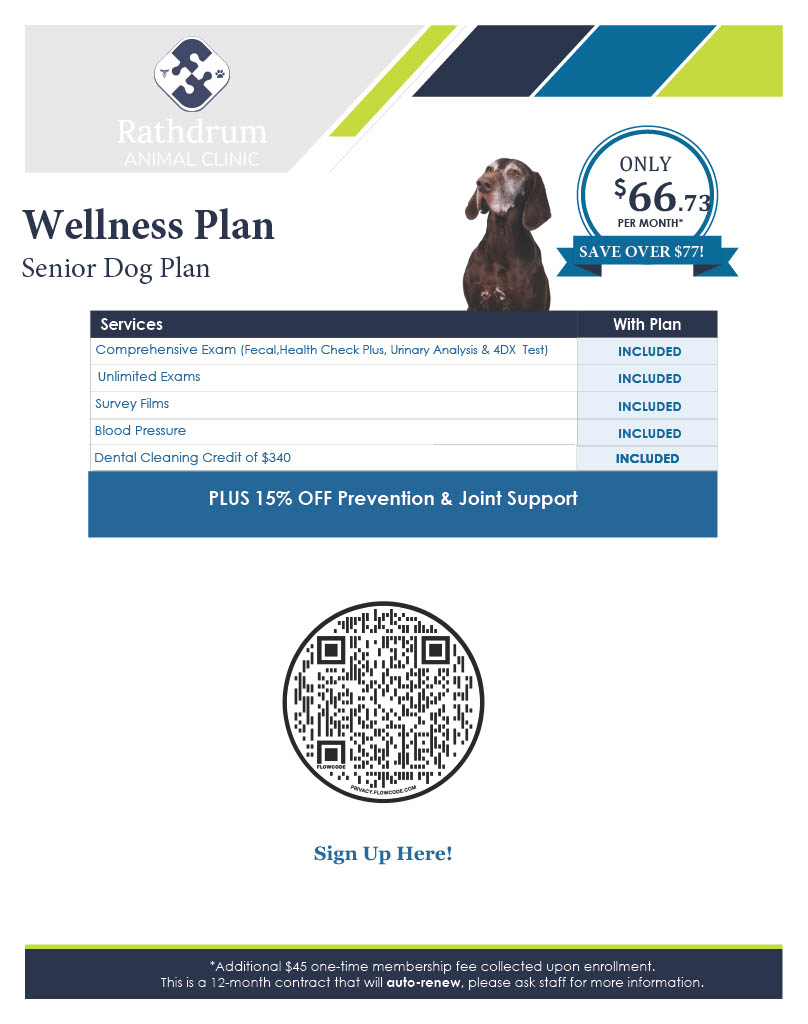
Senior Plan
Feline Plans
Kitten Plan
Adult Plan
Senior Plan
Sign Up Here!
Pet Health
Patient Medical History
Pet Health Library
Pet Health Checker
Pet Health News
How-To Videos
Pet Insurance Info
Online Store
Pet Page
Pet Records Registration
Pet Records Sign-in
Online Pharmacy
Contact
Patient Medical History Form
Medical History to be entered before appointment.
Owner Name
*
Phone
*
Email
*
Patient Name
*
Appointment Date
*
Reason for Visit
*
Does your pet have any previous problems or chronic conditions?
*
If yes, describe.
How is your pet's appetite?
*
Normal
Increased
Decreased
How is your pet's water intake?
*
Normal
Increased
Decreased
How is your pet's urination?
*
Normal
Increased
Decreased
Change in Color
Change in Odor
Other
Is your pet having diarrhea?
*
If yes, for how long?
Has your pet been vomiting?
*
If yes, how often and for how long?
How is your pet's activity level?
*
Normal
Increased
Decreased
Does your pet have any mobility issues?
*
Walking, Standing, Running, etc.
Have you noticed any changes in your pet's behavior?
*
If yes, describe.
Has your pet been sneezing, coughing, or had any other respiratory issues?
*
If yes, describe.
Does your pet have any issues with their Eyes, Mouth, Ears, Skin?
*
If yes, describe.
Is your pet currently taking any medications or supplements?
*
If yes, which ones?
What, How Much, and How Often do you feed your pet?
*
Type of food, 1 cup, 2 cups, Once daily, Twice daily, Free feed, Etc.
Do you travel with you pet or have they ever been away from the North Idaho area?
*
If yes, where?
Do you take your pet to a boarding or grooming facility, dog park, pet store, etc.?
*
How much time does your pet spend indoors vs. outdoors?
*
Is your pet currently on Flea, Tick, and/or Heartworm Prevention?
*
Is yes, what type?
Are there any topics that you would like to discuss at your visit?
*
Δ
New Clients
Practice Policies
Take A Tour
Pet Insurance
About Us
Career Opportunities
Services
Surgical Services
Medical Services
Anesthesia and Patient Monitoring
Preventive Services
Wellness and Vaccination Programs
Additional Services
Wellness Plans
Canine Plans
Puppy Plan
Adult Plan w/ Prevention
Adult Plan w/ Dental Credit
Senior Plan
Feline Plans
Kitten Plan
Adult Plan
Senior Plan
Sign Up Here!
Pet Health
Patient Medical History
Pet Health Library
Pet Health Checker
Pet Health News
How-To Videos
Pet Insurance Info
Online Store
Pet Page
Pet Records Registration
Pet Records Sign-in
Online Pharmacy
Contact
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}